Soft liners improve comfort, suspension, and skin protection for prosthetic users. For most myoelectric hand users, they’ve historically come with a catch: the electrodes need direct skin contact that a liner prevents.
Soft liners have been used in lower limb prosthetics for decades. In upper limb prosthetics, adoption has grown but for users of myoelectric hands, a long-standing obstacle has prevented many patients from accessing the same comfort benefits: the liner sits between the skin and the electrodes that the control system depends on.
This isn’t a minor inconvenience. It’s a clinical trade-off that forces many patients and clinicians to choose between comfort and reliable control and until recently, the options for resolving that trade-off were limited and technically demanding.
Why Liners Matter for Upper Limb Users
The interface between the residual limb and the socket is one of the most consequential factors in long-term prosthetic use. Even a well-designed prosthetic hand becomes difficult to use consistently if the socket causes discomfort, skin breakdown, or inconsistent fit across the course of a day.
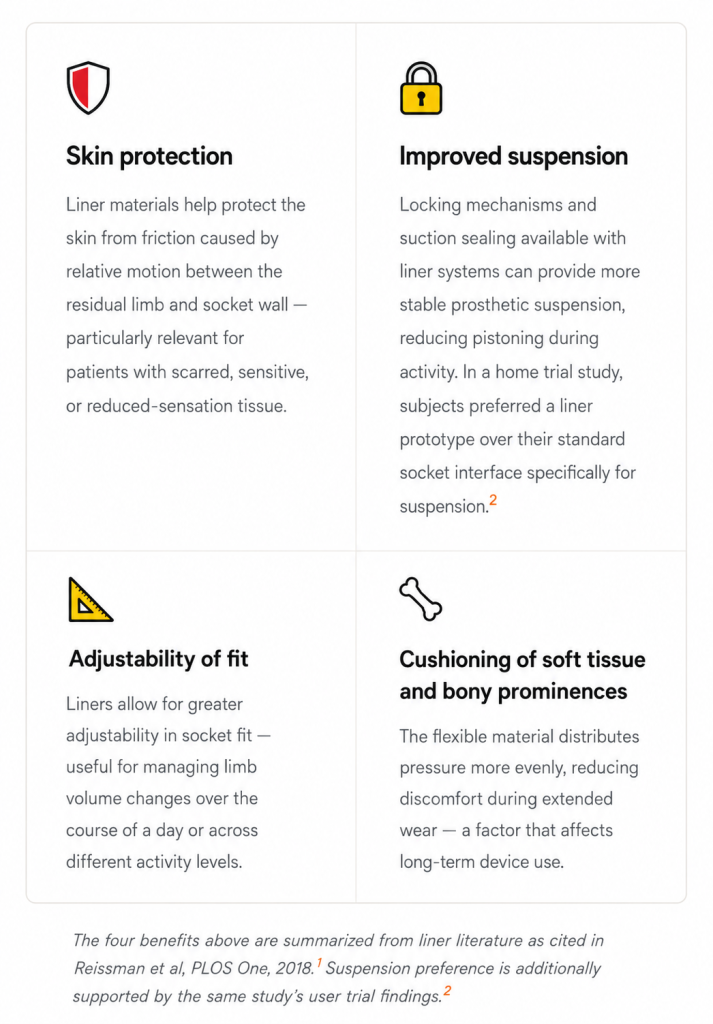
Soft liners, typically made from silicone, urethane, or thermoplastic elastomeric materials, are reported to offer several clinical benefits that address common socket fit challenges.1
Despite these benefits, upper limb myoelectric users cannot wear a liner because the EMG electrode must touch the skin to capture the myoelectric signal. Therefore, upper limb users miss out on the comfort and suspension benefits of the liner, while also not being able to use prosthetic socks for limb volume management.3
The Core Problem: Electrodes Need Skin Contact
The fundamental conflict
Traditional myoelectric systems depend on electrodes embedded inside the socket making direct contact with the skin surface. These electrodes detect the small electrical signals produced by muscle contractions and translate them into prosthetic hand commands.
A liner inserted between the socket and the residual limb physically breaks that contact. The electrode can no longer read the muscle signal through the liner material, and control either fails entirely or becomes unreliable. This is not a solvable problem within the constraints of a socket-embedded electrode architecture. It’s a structural limitation of the design itself.
The clinical consequence is that many myoelectric users who would benefit from a liner, patients with skin integrity concerns, volume fluctuation, or discomfort with hard socket interfaces, have had to go without one. And the workarounds that do exist have typically involved compromises of their own.
How the Field Has Tried to Solve It
Several approaches have been developed over the years to allow liner use with myoelectric systems. Each has moved in a useful direction, but each also carries trade-offs that have limited broader clinical adoption.
A Different Starting Point: Sensing Outside the Socket
A different approach is to remove the electrodes from the socket entirely.
When signal acquisition happens outside the socket, through a wearable sensor band worn on the residual limb, transmitting wirelessly to the prosthetic hand, the liner-electrode conflict doesn’t arise, because there are no socket-embedded electrodes to conflict with.

How Vulcan Myoband approaches this
Wireless sensing, worn outside the socket
The Vulcan Myoband is worn as a wearable sensor band on the upper arm or forearm, outside the prosthetic socket, not inside it. It captures muscle signals and transmits control commands wirelessly to the prosthetic hand via Bluetooth Low Energy (BLE).
Because the Myoband operates independently of the socket, the socket interior can be fabricated with a soft liner without affecting signal acquisition. The patient dons the Myoband, rolls on the liner and socket over it, and the system continues to function — no electrode modification of the liner required, no holes, no specialized manufacturing steps.
This doesn’t eliminate the need for careful sensor placement or calibration. Those remain important for reliable control. But it does remove the structural conflict between liner use and myoelectric control that has historically required workarounds.
It is worth noting that this approach involves trade-offs of its own. A wearable external band adds a donning step and requires consistent positioning on the limb.
The clinical suitability of any approach, socket-embedded, liner-integrated, or wearable external, will depend on the individual patient’s anatomy, activity level, and clinical context. What changes with an external wearable is that the liner question becomes independent of the electrode question, giving clinicians more flexibility to address both on their own terms.
What This Means Clinically
For CPOs working with patients who have skin integrity concerns, volume fluctuation, or significant discomfort with hard socket interfaces, the liner question is a real and recurring clinical consideration.
The field has been working on it for years, through liner modifications, embedded electrode systems, and now wireless architectures, and the solutions are becoming more clinically practical.
The underlying question remains worth keeping in mind: if a patient would benefit from a liner, what would it take to give them one without compromising their myoelectric control? The answer increasingly depends less on modifying the liner to accommodate the electrode, and more on rethinking where the electrode needs to be in the first place.
Learn more about how the Vulcan Myoband’s wearable, socket-independent design supports a wider range of fitting configurations.
1. Reissman T, Halsne E, Lipschutz R, Miller L, Kuiken T. “A novel gel liner system with embedded electrodes for use with upper limb myoelectric prostheses.” PLOS One, June 2018. DOI: 10.1371/journal.pone.0198934 — Benefits of liners (skin protection, cushioning, suspension, adjustability) are cited from general liner literature within this paper’s introduction, not primary findings of this study.
2. Reissman et al., 2018 (same as ref 1). Direct finding from 8-subject home trial: “Subjects preferred the liner prototype (p = 0.008) over their own system in the clinical areas of comfort, suspension, function, and, especially, ease of use.”
3. ASTERISK Study Protocol. ClinicalTrials.gov NCT06821412. “Wireless Prosthetic Control Effectiveness Study.” Accessed June 2026. Source of quote: “upper limb prosthesis users with myoelectric control cannot wear a liner as the electromyogram (EMG) electrode must touch the skin to transduce the myoelectric signal.”
4. Cited approaches (piercing liner with electrode domes; cutting holes in liner) documented in Reissman et al. 2018 introduction, referencing earlier clinical literature on liner modification approaches.