No two patients produce the same EMG signal. Yet many myoelectric fitting workflows still treat signal calibration as a checkbox rather than a clinical decision with predictable consequences for control reliability and device.
Calibration is where the prosthetic control system learns what a specific patient’s muscle signals actually look like. Done well, it produces a device that responds predictably to deliberate commands and ignores incidental muscle activity. Done poorly or skipped in favour of default settings, it produces a device that feels unreliable, unpredictable, or simply too hard to use consistently.
The gap between these two outcomes is not a function of the hardware or the myoelectric hand. It’s a function of how well the control system has been configured to the individual patient in front of the clinician.
Why Individual Variation Makes One-Size Calibration Unreliable
EMG signals are not standardised across patients. The amplitude, timing, and quality of the signals a person generates depend on a range of individual factors that vary significantly between patients, and within the same patient over time. Applying a fixed or population-average calibration to this variation produces control behaviour that fits no one particularly well.
01. Muscle mass and composition
Patients with greater muscle mass or more superficial muscle bellies tend to generate higher-amplitude signals. Patients with atrophy, long-term limb loss, or complex tissue conditions may produce significantly lower amplitudes. A calibration designed for one produces the wrong sensitivity for the other.
02. Voluntary control experience
New prosthetic users often produce inconsistent, variable signals as they learn to isolate and control residual muscle contractions. Experienced users may have well-established, reproducible patterns. Early calibration for a new user needs to accommodate inconsistency; later calibration can take advantage of the improved signal quality that develops with practice.
03. Residual limb condition
Scar tissue, oedema, skin integrity issues, and limb volume fluctuation all affect signal quality and consistency. Two patients with the same amputation level and the same prosthetic hand may require very different calibration approaches because their residual limbs present entirely different signal environments.
04. Signal site location
The specific location where a usable signal is found varies between patients and cannot be reliably predicted from anatomy alone. Moving even a small distance from the optimal site changes signal characteristics enough to require a different calibration response.
05. Fatigue and daily variation
Signal amplitude in the same patient varies across the day as muscles fatigue, perspiration affects electrode contact, and limb volume changes. A calibration that works well in the morning fitting session may produce different control behaviour by the end of a working day.
06. Contralateral limb use
In bilateral amputees or patients who rely heavily on compensatory upper body movement, crosstalk from muscles not intended to generate commands can introduce noise into the signal environment, requiring calibration settings that are more conservative to avoid false activations.
These sources of variation don’t resolve on their own. They require active clinical attention during the calibration process, and they mean that calibration decisions made without considering the individual patient’s signal profile are likely to produce a suboptimal result.
What Happens When Calibration Isn’t Personalised
The consequences of generic or inadequate calibration appear in predictable patterns, most of which clinicians will recognise from patient feedback and return visit behaviour.
False activations and unintended movement
When calibration sets activation levels too low relative to a patient’s resting muscle activity, the hand responds to signals the patient didn’t intend as commands. This is one of the most commonly reported sources of frustration for myoelectric user. A device that moves when the patient doesn’t want it to, or that can’t be trusted in public settings where unexpected hand movement would be embarrassing.
Non-response to deliberate commands
When activation levels are set too high for a patient’s signal amplitude, which frequently happens with patients who have weaker signals due to atrophy or long-term limb loss, the device doesn’t respond to deliberate contractions. The patient has to over-effort to trigger a response, which is tiring, unreliable, and ultimately discouraging.
Performance degradation across the day
If calibration doesn’t account for signal variation due to fatigue, volume change, and perspiration, the control behaviour that feels acceptable in the morning may become noticeably less reliable by the afternoon. Patients who don’t understand why this happens often attribute it to the device being faulty, rather than recognising it as a calibration and signal quality issue.
Excessive recalibration demand
Patients who return repeatedly for calibration adjustments are often experiencing the downstream effects of initial calibration that wasn’t individualised sufficiently. Each visit addresses the symptom — imprecise control — without necessarily addressing the underlying cause, which is a calibration profile that doesn’t accurately reflect that patient’s signal characteristics.
Device abandonment
Unreliable control is a consistently cited factor in prosthetic device abandonment in the upper limb literature. Patients who cannot trust their device’s response, who experience it as unpredictable rather than responsive to their intent, are less likely to persist with use. Calibration that doesn’t fit the patient is a meaningful contributor to this outcome.
Calibration as Patient-Specific Configuration
Effective myoelectric calibration is patient-specific configuration, not a default setting applied uniformly, and not a one-time event at fitting that is assumed to hold indefinitely. It is a clinical process that benefits from the same systematic attention as other aspects of prosthetic fitting.
A useful framing
The control system learns from calibration. What it learns is constrained by what the clinician provides during that process. If calibration is based on a small number of contractions under ideal static conditions, the system learns a narrow, idealised version of the patient’s signal, one that may not hold up under the variable conditions of daily use. If calibration is based on a broader, more systematic assessment of the patient’s signal across different conditions, the system has a more representative foundation to work from.
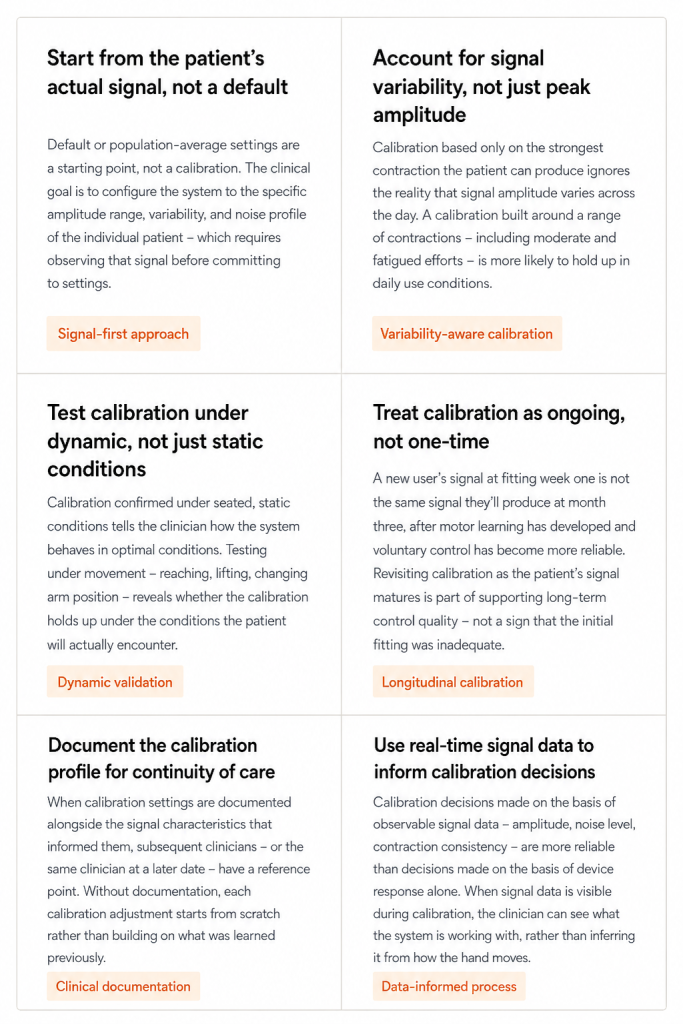
Principles for More Effective Individual Calibration
What This Means for Clinic Workflows
Personalised calibration takes more time than applying a default. For clinics managing high patient volumes, that time pressure is real. However, the downstream cost of inadequate calibration, repeated return visits, frustrated patients, device abandonment, is consistently higher than the upfront investment in a more thorough initial calibration process.
Clinics that treat calibration as a systematic clinical process, with defined steps, documented outputs, and scheduled review, tend to see fewer calibration-related return visits and more consistent patient-reported satisfaction with control reliability. The investment is at fitting; the return is in reduced follow-up burden and better long-term device use.
How Vulcan approaches signal personalisation
The Vulcan Myoband is calibrated individually to each patient’s signal profile through the companion app, the system analyses the patient’s actual muscle activity and configures itself accordingly, rather than applying a fixed starting point. Calibration is designed to take roughly 60 seconds, with the system adapting to where the patient’s signal actually is, including patients with weaker or more variable signals who would present challenges for systems that require stronger, more isolated activation.
Signal data logged during calibration and use can be reviewed at follow-up appointments, giving clinicians a longitudinal view of how a patient’s signal profile evolves, and supporting calibration adjustments grounded in observable data rather than patient self-report alone.
Learn more about how the Myoband’s calibration approach adapts to individual patient signal profiles.