Adaptive control keeps the logic clinicians and patients already know: a lighter contraction opens the hand, a stronger one closes it. It’s intuitive, easy to calibrate, and easy to learn, which is exactly why it remains the most widely used control method in myoelectric prosthetics.
What the Vulcan Myoband changes is how that logic holds up once the patient leaves the clinic and moves through a normal day.

Why EMG Signals Don’t Stay Consistent
The difficulty isn’t the control method itself. It’s that EMG signals naturally vary with fatigue, posture, and electrode contact and a fixed calibration has no way to account for that variation.
A calibration that feels stable in the clinic can behave differently at home, not because anything was set up incorrectly, but because the signal environment has changed. For clinicians, this often means repeated adjustments at follow up. For patients, it can mean a device that feels less predictable than expected, which over time affects confidence and daily use.
How Vulcan Handles It Differently
Vulcan keeps the same basic control logic: lower activation for one action, higher for another because it works and patients understand it. What’s different is how the system holds up once real-world conditions come into play.
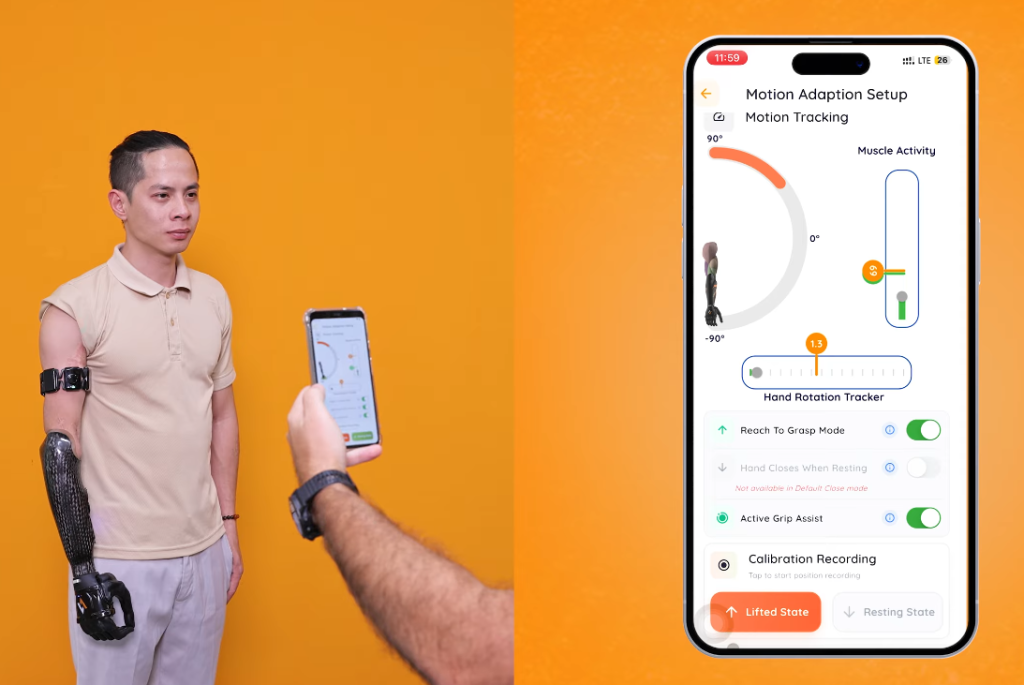
The Myoband doesn’t just read muscle signals in isolation. It also accounts for what the arm itself is doing so the system can tell the difference between a deliberate command and ordinary movement.
Reaching for an object naturally tightens stabilizing muscles something a fixed system can mistake for a command. The Myoband is built to tell the difference, so the hand responds to deliberate movement, not incidental muscle activity.
Same control logic patients are already familiar with, one that adapts to real conditions rather than assuming they stay constant.
What the Data Tells Clinicians Over Time
Because the system tracks performance over time, clinicians build a picture of how each patient’s muscle activity evolves. Are activation levels becoming more consistent? Is the patient needing to contract harder than before?
That kind of longitudinal insight is difficult to get from a conventional setup, where calibration changes happen by feel and little gets recorded systematically. Having it available makes follow-up conversations more grounded and gives rehabilitation teams something concrete to work from when planning training adjustments.
What It Means in Practice
For patients:
Day-to-day control feels more predictable. Fewer unexpected hand movements, less frustration when the device doesn’t respond as expected. The learning curve stays manageable because the underlying logic doesn’t change, it just holds up better under real conditions.
For clinicians and CPOs:
The calibration process stays familiar. The difference is fewer return visits for calibration adjustments, and more confidence that settings will hold between appointments.
For rehabilitation teams
Longitudinal signal data adds a layer of objectivity to recovery tracking that conventional systems don’t easily provide.